
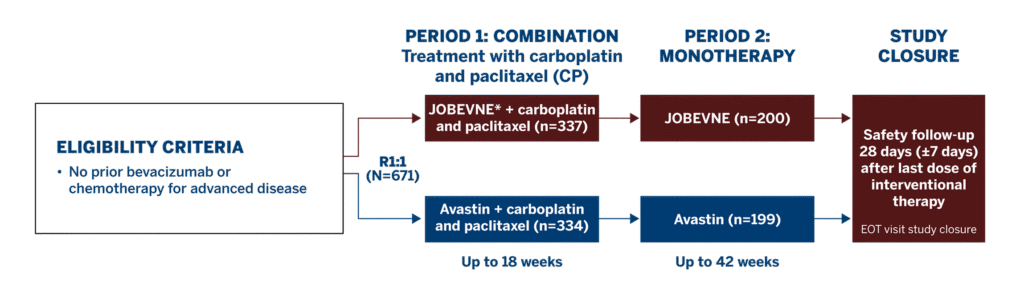
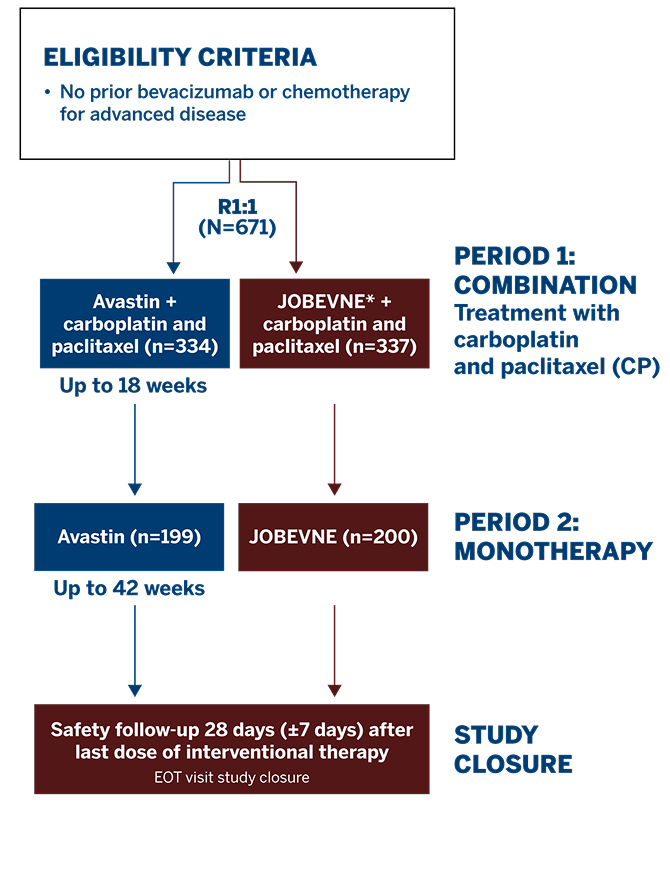
Study Design1
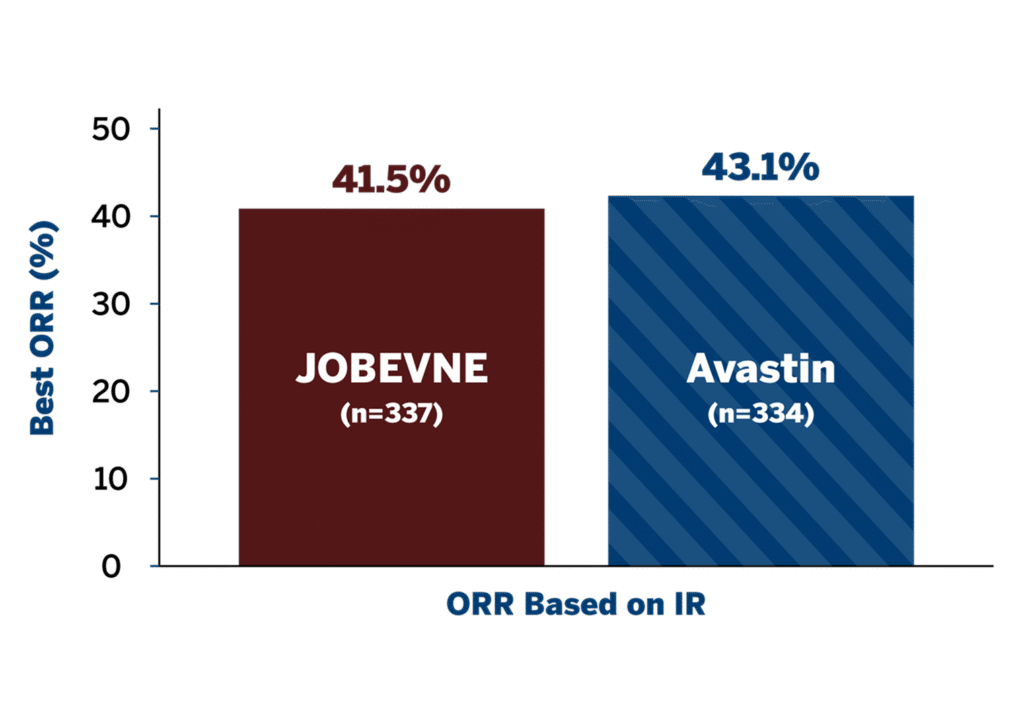
ORR AT WEEK 181
PFS AND OS AT WEEK 421

SAFETY AND IMMUNOGENICITY DATA DEMONSTRATE THE BIOSIMILARITY1
Jobevne™ has achieved all the benchmarks for biosimilarity in efficacy and safety to the reference bevacizumab.1,2
Totality of evidence for JOBEVNE is based on similarity in analytical and clinical data, along with extrapolation of indications to Avastin®.1,2
EFFICACY
This Phase 3 study compared the efficacy and safety of JOBEVNE with Avastin, as first-line treatment for 671 patients with stage IV non-squamous non-small cell lung cancer.
*JOBEVNE was dosed at 15 mg/kg infusion.
†Eligible patients were adults ≥18 years of age.
ECOG=Eastern Cooperative Oncology Group; EOT=end of treatment; R=randomized.
*ORR ratio 90% CI equivalence margin was defined as 0.73 to 1.36, and ORR difference 95% CI equivalence margin was defined as -12.5 to 12.5.
CI=confidence interval; IR=independent review; ORR=overall response rate.
There were no statistically significant differences in PFS at Week 42 between treatment groups.
*No statistically significant difference between treatment arms at 42 weeks; the log-rank test showed a P-value of 0.0906 (IR) between the treatment arms.
†The median OS was not reached in the ITT population at Week 42. According to the log-rank test, the difference between the survival curves for both treatment groups was not statistically significant (P=0.1185).
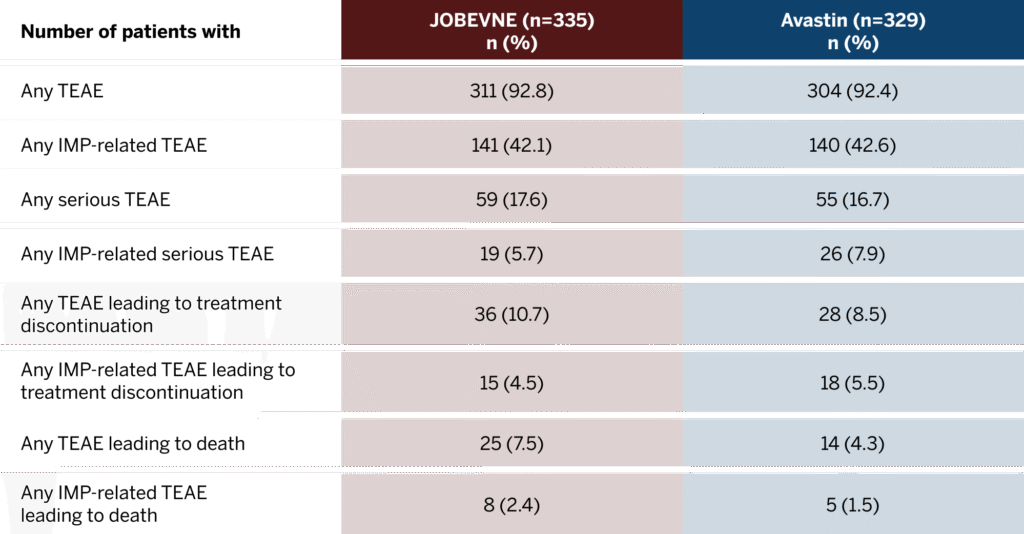
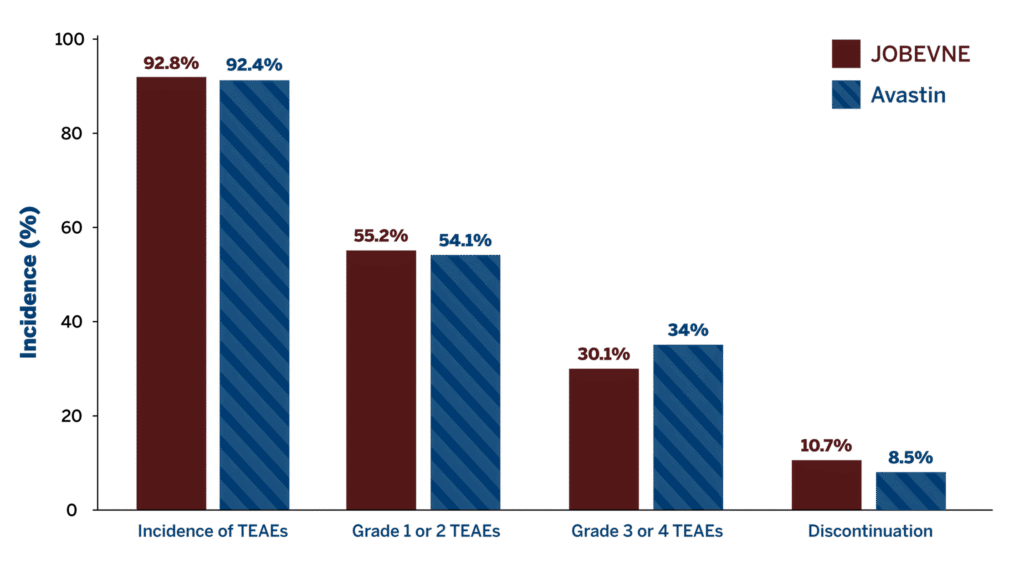
SAFETY
No clinically significant differences were observed between JOBEVNE and Avastin in the incidence of treatment-emergent adverse events (TEAEs) and severity of immune responses.
Overall Incidence of Treatment-Emergent Adverse Events1
Includes Period 1 and Period 2 through Week 42.
Incidence of TEAE in treatment groups1
ADA=anti-drug antibody; IMP=investigational medicinal product; TEAE=treatment-emergent adverse event.
REFERENCES
1. Socinski MA, Waller CF, Idris T, et al. Phase III double-blind study comparing the efficacy and safety of proposed biosimilar MYL-1402O and reference bevacizumab in stage IV non-small-cell lung cancer. Ther Adv Med Oncol. 2021;13:17588359211045845. 2. US Food and Drug Administration. Biosimilars: review and approval. Last updated December 13, 2022. Accessed June 16, 2025. https://www.fda.gov/drugs/biosimilars/review-and-approval
IMPORTANT SAFETY INFORMATION AND INDICATIONS
READ MORE +
SHOW LESS -
IMPORTANT SAFETY INFORMATION
JOBEVNE can cause serious side effects, including:
Gastrointestinal (GI) perforations and fistulae: Serious, and sometimes fatal, gastrointestinal perforation occurred at a higher incidence in patients receiving bevacizumab products compared to patients receiving chemotherapy. The incidence ranged from 0.3% to 3% across clinical studies, with the highest incidence in patients with a history of prior pelvic radiation. Serious fistulae ranged from < 1% to 1.8% across clinical studies, with the highest incidence in patients with cervical cancer. Avoid JOBEVNE in patients with ovarian cancer who have evidence of recto-sigmoid involvement by pelvic examination or bowel involvement on CT scan or clinical symptoms of bowel obstruction. Discontinue in patients who develop gastrointestinal perforation, tracheoesophageal fistula, or any Grade 4 fistula. Discontinue in patients with fistula formation involving any internal organ.
Surgery and Wound Healing Complications: The incidence of surgery and wound healing complications, including serious and fatal complications, was increased in patients receiving bevacizumab products. In patients who experience wound healing complications during treatment, withhold JOBEVNE until adequate wound healing. Do not use JOBEVNE for at least 28 days following major surgery, to allow time for the wound to heal. Discontinue JOBEVNE in patients who develop necrotizing fasciitis.
Hemorrhage: Severe or fatal hemorrhage including hemoptysis, gastrointestinal bleeding, hematemesis, CNS hemorrhage, epistaxis, and vaginal bleeding, occurred up to 5-fold more frequently in patients receiving bevacizumab products vs chemotherapy alone. Discontinue JOBEVNE in patients who develop a Grades 3-4 hemorrhage.
Arterial Thromboembolic Events: Serious, sometimes fatal, arterial thromboembolic events (ATE) including cerebral infarction, transient ischemic attacks, myocardial infarction, and angina, occurred at a higher incidence in patients receiving bevacizumab vs chemotherapy. Discontinue JOBEVNE in patients who develop severe ATE. The safety of reinitiating bevacizumab products after an ATE is resolved is not known.
Venous Thromboembolic Events: An increased risk of venous thromboembolic events (VTE) was observed across clinical studies. Discontinue JOBEVNE in patients with a Grade 4 VTE, including pulmonary embolism.
Hypertension: Severe hypertension occurred at a higher incidence in patients receiving bevacizumab products as compared to chemotherapy alone. Monitor blood pressure every two to three weeks during treatment with JOBEVNE. Treat with appropriate anti-hypertensive therapy and monitor blood pressure regularly. Discontinue in patients who develop hypertensive crisis or hypertensive encephalopathy.
Posterior Reversible Encephalopathy Syndrome (PRES): PRES was reported in < 0.5% of patients across clinical studies. Discontinue JOBEVNE in patients who develop PRES.
Renal Injury and Proteinuria: The incidence and severity of proteinuria was higher in patients receiving bevacizumab as compared to patients receiving chemotherapy. Nephrotic syndrome occurred in < 1% of patients receiving bevacizumab products across clinical studies, in some instances with fatal outcome. Discontinue JOBEVNE in patients who develop nephrotic syndrome.
Infusion-related reactions: Infusion-related reactions reported across clinical studies and post marketing experience include hypertension, hypertensive crises associated with neurologic signs and symptoms, wheezing, oxygen desaturation, Grade 3 hypersensitivity, anaphylactoid/anaphylactic reactions, chest pain, headaches, rigors, and diaphoresis. In clinical studies, infusion-related reactions with the first dose of bevacizumab products occurred in < 3% of patients and severe reactions occurred in 0.4% of patients. Decrease the rate of infusion for mild, clinically insignificant infusion-related reactions. Interrupt the infusion in patients with clinically significant infusion-related reactions and consider resuming at a slower rate following resolution. Discontinue JOBEVNE in patients who develop a severe infusion-related reaction and administer appropriate medical therapy.
Embryo-Fetal Toxicity: Bevacizumab products may cause fetal harm when administered to pregnant women. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with JOBEVNE and for 6 months after the last dose.
Ovarian Failure: The incidence of ovarian failure was 34% vs 2% in premenopausal women receiving bevacizumab with chemotherapy vs chemotherapy alone for adjuvant treatment of a solid tumor. Inform females of reproductive potential of the risk of ovarian failure prior to initiating JOBEVNE.
Congestive Heart Failure (CHF): JOBEVNE is not indicated for use with anthracycline-based chemotherapy. Discontinue JOBEVNE in patients who develop CHF.
Most common adverse reactions incidence (incidence >10%): epistaxis, headache, hypertension, rhinitis, proteinuria, taste alteration, dry skin, hemorrhage, lacrimation disorder, back pain and exfoliative dermatitis.
Across clinical studies, bevacizumab was discontinued in 8% to 22% of patients because of adverse reactions.
Most Common Adverse Reactions by Indication
Metastatic Colorectal Cancer:
First-Line Non-Squamous Non–Small Cell Lung Cancer (NSCLC)
Recurrent Glioblastoma
Metastatic Renal Cell Carcinoma
Persistent, Recurrent, or Metastatic Cervical Cancer
Epithelial Ovarian, Fallopian Tube or Primary Peritoneal Cancer
INDICATIONS
Metastatic Colorectal Cancer (mCRC)
JOBEVNE combined with intravenous fluorouracil-based chemotherapy for first- or second-line treatment of patients with mCRC.
JOBEVNE combined with fluoropyrimidine-irinotecan- or fluoropyrimidine-oxaliplatin-based chemotherapy for the second-line treatment of patients with mCRC who have progressed on a first-line treatment containing bevacizumab.
Limitations of Use: JOBEVNE is not approved for use if surgery was used as the primary treatment in patients with colon cancer which has not spread to other parts of the body.
First-Line Non-Squamous Non–Small Cell Lung Cancer (NSCLC):
JOBEVNE combined with carboplatin and paclitaxel is approved for first-line treatment in patients with unresectable, locally advanced, recurrent or metastatic NSCLC.
Recurrent Glioblastoma (rGBM):
JOBEVNE is approved to treat rGBM in adults.
Metastatic Renal Cell Carcinoma (mRCC):
JOBEVNE combined with interferon alfa, is approved to treat mRCC.
Persistent, Recurrent or Metastatic Cervical Cancer (CC):
JOBEVNE combined with paclitaxel and cisplatin or paclitaxel and topotecan, is approved to treat patients with persistent, recurrent, or metastatic cervical cancer.
Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer:
IMPORTANT SAFETY INFORMATION AND INDICATIONS
IMPORTANT SAFETY INFORMATION
JOBEVNE can cause serious side effects, including:
Gastrointestinal (GI) perforations and fistulae: Serious, and sometimes fatal, gastrointestinal perforation occurred at a higher incidence in patients receiving bevacizumab products compared to patients receiving chemotherapy. The incidence ranged from 0.3% to 3% across clinical studies, with the highest incidence in patients with a history of prior pelvic radiation. Serious fistulae ranged from < 1% to 1.8% across clinical studies, with the highest incidence in patients with cervical cancer. Avoid JOBEVNE in patients with ovarian cancer who have evidence of recto-sigmoid involvement by pelvic examination or bowel involvement on CT scan or clinical symptoms of bowel obstruction. Discontinue in patients who develop gastrointestinal perforation, tracheoesophageal fistula, or any Grade 4 fistula. Discontinue in patients with fistula formation involving any internal organ.
Surgery and Wound Healing Complications: The incidence of surgery and wound healing complications, including serious and fatal complications, was increased in patients receiving bevacizumab products. In patients who experience wound healing complications during treatment, withhold JOBEVNE until adequate wound healing. Do not use JOBEVNE for at least 28 days following major surgery, to allow time for the wound to heal. Discontinue JOBEVNE in patients who develop necrotizing fasciitis.
Hemorrhage: Severe or fatal hemorrhage including hemoptysis, gastrointestinal bleeding, hematemesis, CNS hemorrhage, epistaxis, and vaginal bleeding, occurred up to 5-fold more frequently in patients receiving bevacizumab products vs chemotherapy alone. Discontinue JOBEVNE in patients who develop a Grades 3-4 hemorrhage.
Arterial Thromboembolic Events: Serious, sometimes fatal, arterial thromboembolic events (ATE) including cerebral infarction, transient ischemic attacks, myocardial infarction, and angina, occurred at a higher incidence in patients receiving bevacizumab vs chemotherapy. Discontinue JOBEVNE in patients who develop severe ATE. The safety of reinitiating bevacizumab products after an ATE is resolved is not known.
Venous Thromboembolic Events: An increased risk of venous thromboembolic events (VTE) was observed across clinical studies. Discontinue JOBEVNE in patients with a Grade 4 VTE, including pulmonary embolism.
Hypertension: Severe hypertension occurred at a higher incidence in patients receiving bevacizumab products as compared to chemotherapy alone. Monitor blood pressure every two to three weeks during treatment with JOBEVNE. Treat with appropriate anti-hypertensive therapy and monitor blood pressure regularly. Discontinue in patients who develop hypertensive crisis or hypertensive encephalopathy.
Posterior Reversible Encephalopathy Syndrome (PRES): PRES was reported in < 0.5% of patients across clinical studies. Discontinue JOBEVNE in patients who develop PRES.
Renal Injury and Proteinuria: The incidence and severity of proteinuria was higher in patients receiving bevacizumab as compared to patients receiving chemotherapy. Nephrotic syndrome occurred in < 1% of patients receiving bevacizumab products across clinical studies, in some instances with fatal outcome. Discontinue JOBEVNE in patients who develop nephrotic syndrome.
Infusion-related reactions: Infusion-related reactions reported across clinical studies and post marketing experience include hypertension, hypertensive crises associated with neurologic signs and symptoms, wheezing, oxygen desaturation, Grade 3 hypersensitivity, anaphylactoid/anaphylactic reactions, chest pain, headaches, rigors, and diaphoresis. In clinical studies, infusion-related reactions with the first dose of bevacizumab products occurred in < 3% of patients and severe reactions occurred in 0.4% of patients. Decrease the rate of infusion for mild, clinically insignificant infusion-related reactions. Interrupt the infusion in patients with clinically significant infusion-related reactions and consider resuming at a slower rate following resolution. Discontinue JOBEVNE in patients who develop a severe infusion-related reaction and administer appropriate medical therapy.
Embryo-Fetal Toxicity: Bevacizumab products may cause fetal harm when administered to pregnant women. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with JOBEVNE and for 6 months after the last dose.
Ovarian Failure: The incidence of ovarian failure was 34% vs 2% in premenopausal women receiving bevacizumab with chemotherapy vs chemotherapy alone for adjuvant treatment of a solid tumor. Inform females of reproductive potential of the risk of ovarian failure prior to initiating JOBEVNE.
Congestive Heart Failure (CHF): JOBEVNE is not indicated for use with anthracycline-based chemotherapy. Discontinue JOBEVNE in patients who develop CHF.
Most common adverse reactions incidence (incidence >10%): epistaxis, headache, hypertension, rhinitis, proteinuria, taste alteration, dry skin, hemorrhage, lacrimation disorder, back pain and exfoliative dermatitis.
Across clinical studies, bevacizumab was discontinued in 8% to 22% of patients because of adverse reactions.
Most Common Adverse Reactions by Indication
Metastatic Colorectal Cancer:
First-Line Non-Squamous Non–Small Cell Lung Cancer (NSCLC)
Recurrent Glioblastoma
Metastatic Renal Cell Carcinoma
Persistent, Recurrent, or Metastatic Cervical Cancer
Epithelial Ovarian, Fallopian Tube or Primary Peritoneal Cancer
INDICATIONS
Metastatic Colorectal Cancer (mCRC)
Limitations of Use: JOBEVNE is not approved for use if surgery was used as the primary treatment in patients with colon cancer which has not spread to other parts of the body.
First-Line Non-Squamous Non–Small Cell Lung Cancer (NSCLC):
JOBEVNE combined with carboplatin and paclitaxel is approved for first-line treatment in patients with unresectable, locally advanced, recurrent or metastatic NSCLC.
Recurrent Glioblastoma (rGBM):
JOBEVNE is approved to treat rGBM in adults.
Metastatic Renal Cell Carcinoma (mRCC):
JOBEVNE combined with interferon alfa, is approved to treat mRCC.
Persistent, Recurrent or Metastatic Cervical Cancer (CC):
JOBEVNE combined with paclitaxel and cisplatin or paclitaxel and topotecan, is approved to treat patients with persistent, recurrent, or metastatic cervical cancer.
Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer:
Biocon Biologics Inc. assumes no responsibility for and makes no warranties or representation of any kind as to the accuracy, currency, or completeness of any information contained in such third-party website, including any third-party social media or mobile application platform. Inclusion of any third-party link on this website does not imply an endorsement or recommendation by Biocon Biologics, and a link to this website from another website does not imply a relationship between Biocon Biologics and any third party. Your use of any such third-party site or platform is at your own risk and will be governed by such third party’s terms and policies (including its privacy policy). Biocon Biologics shall not be liable for any direct, indirect, consequential, incidental or punitive damages arising out of access to, use of, or inability to use such third-party website, or any errors or omissions in the content thereof.
Biocon Biologics Inc. assumes no responsibility for and makes no warranties or representation of any kind as to the accuracy, currency, or completeness of any information contained in such third-party website, including any third-party social media or mobile application platform. Inclusion of any third-party link on this website does not imply an endorsement or recommendation by Biocon Biologics, and a link to this website from another website does not imply a relationship between Biocon Biologics and any third party. Your use of any such third-party site or platform is at your own risk and will be governed by such third party’s terms and policies (including its privacy policy). Biocon Biologics shall not be liable for any direct, indirect, consequential, incidental or punitive damages arising out of access to, use of, or inability to use such third-party website, or any errors or omissions in the content thereof.
Limitations of Use: JOBEVNE is not approved for use if surgery was used as the primary treatment in patients with colon cancer which has not spread to other parts of the body.
JOBEVNE combined with carboplatin and paclitaxel is approved for first-line treatment in patients with unresectable, locally advanced, recurrent or metastatic NSCLC.
JOBEVNE combined with interferon alfa, is approved to treat mRCC.
JOBEVNE combined with paclitaxel and cisplatin or paclitaxel and topotecan, is approved to treat patients with persistent, recurrent, or metastatic cervical cancer.